Schwannoma
Pathology:
T1: isointense or hypointense
T2: heterogeneously hyperintense (Antoni type A: relatively low; Antoni type B: high)
A-densely packed neural and fibrous tissue with little extra cellular fluid
B-loosely arranged tissue with more extra cellular fluid


LOCATION:
- intracranial schwannomas
- cranial nerves: although almost any cranial nerve may be involved, except olfactory nerves and optic nerves which lack sheaths composed of Schwann cells, by far the most commonly involved nerve is the vestibulocochlear nerve (CN VIII)
- non-cranial nerve or intracerebral (very rare)
- intraorbital schwannoma: commonly arise from supraorbital and supratrochlear nerves in the upper anterior orbital cavity 10
- spinal schwannoma
- arising from spinal nerve roots
- trunk
- intercostal nerves: see intercostal nerve schwannoma
- posterior mediastinum
- retroperitoneum
- gastrointestinal schwannoma
- limbs
- especially flexor surfaces (specifically ulnar and peroneal nerves)
29 year old female came for surgical checkup with xray
XRAY:
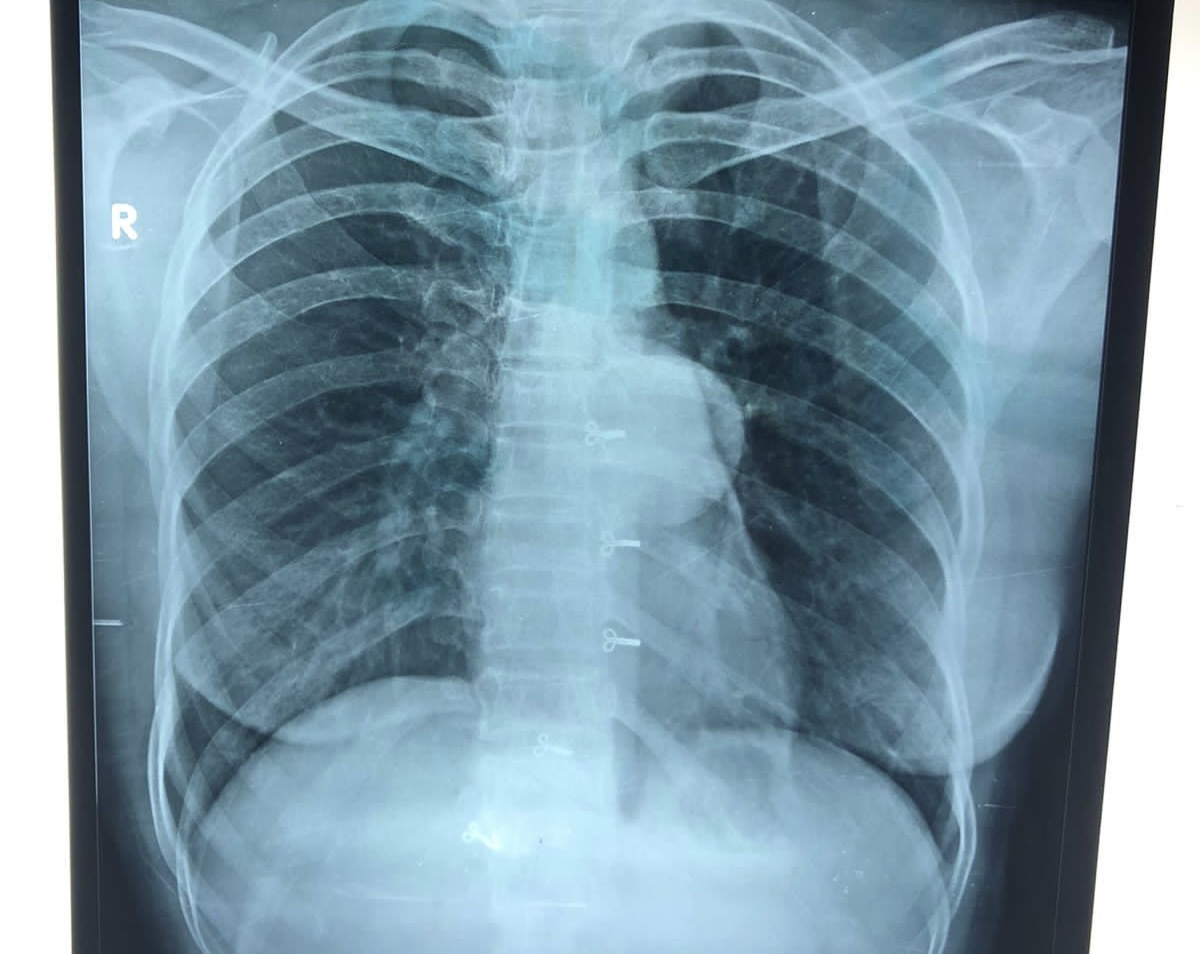
Left margin of the heart is clearly seen through the lesion
-Posterior mediastinal massMri:



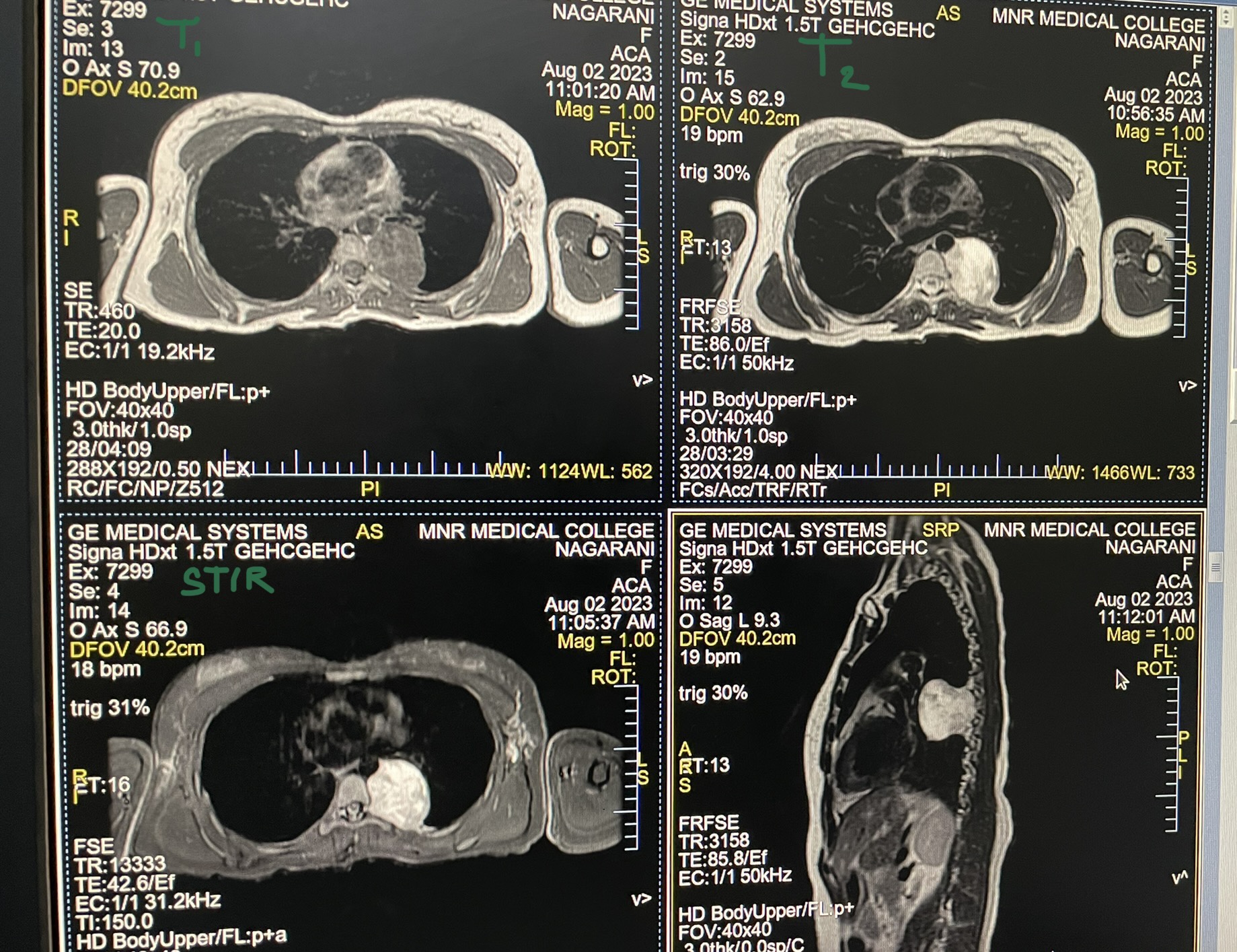
- split-fat sign: the thin peripheral rim of fat best seen on planes along the long axis of the lesion in non-fat-suppressed sequences
- target sign
- peripheral high T2 signal
- central low signal
- rarely seen intracranially
- fascicular sign: multiple small ring-like structures

- extracanalicular extension may result in an "ice cream cone" appearance, presumed to represent tumor growth inwards along a path of least resistance

Comments
Post a Comment